Dr. Casséus: "When the Supply Chain Is the System"
Dr. Alain Casséus, a Partners In Health leader in Haiti, shares a critical perspective on what happens if aid disappears and lifesaving supplies can’t reach the patients who need them
Posted on Apr 9, 2026

Since the Trump administration took office over a year ago, systems of aid that had been built over decades fell into disarray. Resources that had been a lifeline for millions of people around the world disappeared overnight. Organizations like Partners In Health (PIH) rushed to help fill the gaps while advocates and experts appealed to members of Congress to restore foreign aid funding.
This month, a frightening reality emerged: updates from the United States Department of State revealed that national supply chains are in immediate danger. Dr. Alain Casséus, infectious diseases division chief and principal investigator for the PEPFAR Project for Zanmi Lasante, PIH's sister organization in Haiti, knows the country will feel the effects of a supply chain collapse immediately. To explain this rapidly approaching change, he shares his firsthand perspective on what would happen to the people of Haiti if these systems fail. Below is a piece Casséus originally published on Substack.
⎯
When the Supply Chain Is the System
There is a warehouse in Port-au-Prince. It sits in the Fleuriot Industrial Park, sixty thousand square feet of pharmaceutical-grade storage, climate-controlled on one side, ambient on the other, with an 82-square-meter cold room holding reagents and biologicals at precisely 2-8°C. A backup Thermo King container stands ready for overflow. On any given day, eight to fifteen million dollars’ worth of antiretrovirals, viral load reagents, HIV test kits, pediatric drug suspensions, and laboratory supplies are stored there, sorted across roughly four hundred unique product lines. Every month, some six hundred dispatches leave this building bound for 272 health facilities scattered across Haiti’s ten departments—clinics in the Artibonite valley, hospitals in the Central Plateau, treatment centers in the southern peninsula, faith-based dispensaries in places most maps don’t bother naming.
Few people outside the global health supply chain world have heard of this warehouse. It has no public profile. It does not appear in foreign policy debates. It is not the kind of thing that trends.
And yet, for roughly 140,000 Haitians living with HIV, and for the thousands more diagnosed with tuberculosis each year, this warehouse—and the system that feeds and empties it—is the single most important piece of infrastructure in the country. More important than the shuttered parliament. More important than the airport, which hasn’t handled a commercial flight since November 2024. More importantly, in the most literal sense, than anything the Haitian state itself operates.
That system is called GHSC-PSM. It is run by Chemonics International under a USAID contract. And it is being shut down.
I. A System You Only Notice When It Disappears
The full name—Global Health Supply Chain Program, Procurement and Supply Management—is the kind of acronym-heavy bureaucratic title designed to convey seriousness while discouraging curiosity. It tells you nothing about what the program actually does, which is this: it buys the medicines that keep HIV-positive Haitians alive, stores them in controlled conditions, and delivers them to the clinics where patients show up each month hoping the drugs are there.
This sounds simple. It is not. In most PEPFAR countries, GHSC-PSM handles procurement and delivers to the national medical stores. The government takes it from there. Haiti does not have a national medical store system for HIV commodities. There is no “from there.” GHSC-PSM manages the entire chain: international procurement under negotiated global contracts, customs clearance at Port-au-Prince, warehousing at Fleuriot, and last-mile delivery via contracted local trucking companies to every single facility. It quantifies demand. It forecasts need. It manages the cold chain. It runs the electronic logistics management information system—SYGDOCC—that tells everyone what is where.
Among the 73 countries where GHSC-PSM operates, Haiti is one of roughly twenty where the program manages end-to-end distribution. Among those twenty, it is the one where the gap between what the program provides and what the country can provide on its own is widest. The Center for Global Development calculated that USAID supply chain funding to Haiti — $23.7 million per year — represents 37% of the country’s total domestic government health expenditure.
That is the highest ratio of any country in the world.
The government of Haiti, for its part, allocates roughly $250,000 per year to HIV, TB, and malaria combined. After the PEPFAR crisis began in January 2025, this was increased to a $900,000 national budget line for ARV procurement—a meaningful gesture, representing approximately 3.8% of the annual USAID contribution it would need to replace.
There is a temptation, when confronting numbers like these, to reach for the word “dependency”—as though the problem were one of weak national character or misplaced paternalism. But dependency implies a relationship that could be otherwise. What we are describing in Haiti is something closer to substitution. The supply chain was never Haitian. It was always American — designed, funded, operated, and managed by a Washington-based contractor under a USAID contract. The question was never when Haiti would take it over. The question was whether anyone would notice when it stopped.
II. Who Pays, Who Delivers, Who Disappears
To understand why the GHSC-PSM wind-down matters so much, you need to understand the architecture it sits inside: an architecture of almost total external dependence that has been decades in the making.
PEPFAR contributes approximately 79% of Haiti’s national HIV response. The Global Fund provides about 18%. The Government of Haiti covers roughly 2%. Under COP23, PEPFAR allocated approximately $112 million annually to Haiti, with $8.76 million earmarked for ARVs, $6.28 million for HIV laboratory services, including viral load and early infant diagnosis, and smaller amounts for supply chain management and lab systems strengthening.
The Global Fund’s current grant (Grant Cycle 7, 2024-2026) provides approximately $82 million for HIV and TB combined, with World Vision International as the principal recipient and GHESKIO, PIH/Zanmi Lasante, and the national programs as sub-recipients. A separate $7.9 million goes to health systems strengthening through MSPP’s project management unit.
The system operates on two parallel tracks that have never fully merged, despite years of aspiration to do so. Track one: HIV commodities flow through GHSC-PSM—international procurement, customs, Fleuriot Warehouse, 3PL delivery to facilities. This track bypasses PROMESS, Haiti’s national essential medicines program, entirely. Track two: TB and malaria commodities flow through the Global Fund to PROMESS, then through ten departmental depots to facilities. More than twenty distinct actors are involved across both tracks.
The implementing partners who depend on this machinery are organizations that have spent decades building Haiti’s HIV response from nothing. PIH, through its Haitian sister organization Zanmi Lasante, runs 13 hospitals and health centers in Plateau Central and Bas Artibonite, among the country’s most remote regions. PIH launched one of the world’s first ARV treatment programs in a resource-limited setting in 1998, before PEPFAR existed. They have achieved near-95-95-95 targets in their catchment areas, making Plateau Central one of the most successful HIV programs in the Caribbean. GHESKIO, the oldest AIDS research and treatment center in the developing world, serves metropolitan Port-au-Prince. Over half its staff have been displaced by gang violence in the past three years.
None of these organizations procure their own ARVs. None operate warehouses. They all receive their HIV commodities from the Fleuriot Warehouse, delivered by GHSC-PSM’s contracted truckers.
When those trucks stop coming—and they will—there is nothing behind them.
III. The Particular Genius of Last-Mile Delivery in a War Zone
Perhaps the most quietly remarkable thing GHSC-PSM has done in Haiti is something that, by its nature, resists celebration: it has kept delivering medicines in conditions that would have defeated most logistics operations on earth.
In early 2024, when the Viv Ansanm gang coalition launched coordinated assaults across Port-au-Prince, shutting down the port and the airport and seizing control of every major road artery, GHSC-PSM’s Haiti team arranged something unprecedented. They partnered with the World Food Programme to transport ARVs from Port-au-Prince by barge — sea transport around the coast to reach distribution points that could no longer be reached by road. By the end of the quarter, almost all 270 health centers had received vital supplies valued at $2.7 million.
This kind of adaptive logistics (improvising maritime routes under active armed conflict) is not a function you can write into a transition plan. It is the product of institutional knowledge accumulated over a decade: which roads are passable on which days, which local truckers have relationships with which armed groups, where the alternate routes are, when to use barges, when to wait. It is the kind of knowledge that lives in people, not systems, and that disappears when those people leave.
The Fleuriot Warehouse itself tells a similar story. Run by an all-female management team recognized for near-perfect stock accuracy — best-in-class globally within GHSC-PSM — the warehouse handles PEPFAR commodities as well as Global Fund HIV products and supplies for UN agencies. It is, in effect, the shared physical infrastructure on which the entire HIV response depends, regardless of which donor funded the pills inside.
For viral load and early infant diagnosis, GHSC-PSM’s 2019 global procurement awards to Abbott, Hologic, and Roche established all-inclusive contracts that brought Haiti’s per-test cost down from roughly $21 to $13.50, with service-level agreements covering instrument uptime, maintenance, and training. No other procurement mechanism on earth offers these terms. They are a function of PEPFAR’s aggregate global volume, over ten million tests per year, which gives Chemonics leverage that no individual country, and no alternative pooled procurement platform, can replicate.
When people talk about “replacing” GHSC-PSM, they are usually talking about procurement — can the Global Fund buy ARVs? Can PAHO purchase medicines? The answer to both is yes. But procurement is not the problem. The problem is everything that happens after the medicine arrives in-country. And in Haiti, “everything that happens after” is the entire supply chain.
As Emily Bass, the investigative journalist who has provided the most detailed real-time documentation of GHSC-PSM’s emergency closeout, put it: “None of the existing procurement mechanisms identified as eventual replacements for the US supply chain enterprise provide the range of services, including in-country delivery and logistics, for the commodities that GHSC-PSM supported."
IV. The Country Behind the Supply Chain
There is a reason Haiti is different from every other country in the GHSC-PSM portfolio, and it is not primarily about health systems. It is about the collapse of the conditions that make any system possible.
As of mid-2025, approximately 90% of Port-au-Prince is under the control of the Viv Ansanm coalition: an alliance of formerly rival gangs estimated at 12,000-20,000 members, roughly 3,000 of them heavily armed. Every national road artery passes through gang-controlled territory. Route Nationale 1 north to Cap-Haitien. Route Nationale 2 south to Les Cayes. Route Nationale 3 east to Hinche and the Central Plateau. Blockades, ambushes, and extortion tolls are routine.
The Varreux fuel terminal, where 70% of Haiti’s fuel is stored, has been blockaded by gangs before, for two months in 2022. This matters for cold chains. You cannot keep reagents at 2-8°C without power, and you cannot run generators without diesel, and you cannot get diesel when armed groups control the terminal.
The main port has been “inaccessible due to insecurity” and “unreliable for consistent cargo delivery” since late 2024. International commercial flights to Port-au-Prince have been suspended since November 2024. In a country where 70% of medications are imported, this is an existential threat.
As of February 2025, only 10% of health facilities nationwide were fully operational. In Port-au-Prince, over 60% were closed or non-functional. Nine of forty HIV/TB treatment sites in the capital had shut down. MSF, or Doctors Without Borders, an organization that operates in active war zones as a matter of institutional identity, permanently closed its main Port-au-Prince emergency centre in October 2025 and suspended its Bel-Air clinic in January 2026 after a former volunteer was killed at the entrance.
Forty percent of Haiti’s medical staff had left the country by the end of 2023. MSPP reported 39 kidnappings of doctors in the first half of 2023 alone. A survey found 44% of health workers reported a colleague had been kidnapped in the previous two years. The national ratio of health professionals stands at 6.4 per 10,000 population, against a target of 44.5.
There are 1.4 million internally displaced persons—a record, up 34% since December 2024. Each one a potential treatment interruption. Each one a person who was in care somewhere and is now somewhere else, without medicines, without a clinic, without a chart.
This is the environment in which someone, somewhere, is supposed to design a “transition.”
V. The Transition That Isn’t
Here is what we know about the plan to replace GHSC-PSM in Haiti: there isn’t one, for now.
The GHSC-PSM contract was extended through November 28, 2026, intended as a bridge to the NextGen successor program. Then the Trump administration froze all foreign aid on January 20, 2025. A stop-work order halted all operations on January 24. A limited waiver on February 1 allowed some HIV treatment to resume, but as of February 9, fewer than 10% of surveyed PEPFAR partners had restarted services. PEPFAR’s statutory authorization expired March 25, 2025, without reauthorization—the first time in its history. USAID was formally absorbed into the State Department. Eighty-six percent of USAID staff and contractors were terminated or departed. The FY2026 budget request cut PEPFAR by 40%.
The NextGen PSA HIV/AIDS contract (the roughly $5 billion successor to GHSC-PSM’s core procurement function) was cancelled in August 2025. USAID stated it “no longer has a requirement for the services described." The program being shut down has no designated successor mechanism.
By March 30, 2026, emergency closeout planning had formally begun. An internal Chemonics email documented by Emily Bass laid out the arithmetic of collapse: eight countries facing program halts by April 30, 2026, thirteen more in subsequent months. The State Department simultaneously denied that any direction to cease operations had been issued.
Under the America First Global Health Strategy, the U.S. has been negotiating bilateral MOUs with PEPFAR-recipient countries. By April 6, 2026, twenty-seven countries had signed, totaling at least $20.1 billion for 2026-2030 (Think Global Health, April 2026). All were African nations or a handful of Latin American countries. Haiti is not among them.
The Global Fund Advocates Network confirmed in November 2025 that “MOUs are being drafted by the US Embassy and the MOH in Haiti." But negotiating a bilateral agreement with a government that controls almost none of its national territory, has no fiscal capacity for cofinancing, and is engulfed in armed conflict is, to put it charitably, a hard case.
What about the Global Fund? Its $82 million Haiti grant is active. Its Pooled Procurement Mechanism already handles about 90% of procurement within the grant. But the PPM delivers to port or central stores. It does not manage in-country logistics, warehousing, customs, last-mile delivery, or LMIS—the functions GHSC-PSM performs and that keep the entire system from being just a pile of medicines in a building somewhere. The wambo.org procurement platform has been experiencing performance issues. The grant budget was assembled before USAID withdrew and doesn’t include resources to absorb USAID-funded functions.
PAHO’s Strategic Fund can purchase medicines. But Haiti cannot pre-finance orders. And PAHO does not deliver to facilities.
KFF reviewed eight global pooled procurement mechanisms and concluded that all have “key structural gaps relative to GHSC-PSM’s end-to-end model." The polite way of saying: everyone can buy the drugs, no one can deliver them.
VI. What Fails, and in What Order
Not everything breaks at once. But the sequence matters, because it determines where intervention is most urgent — and where the window is already closing.
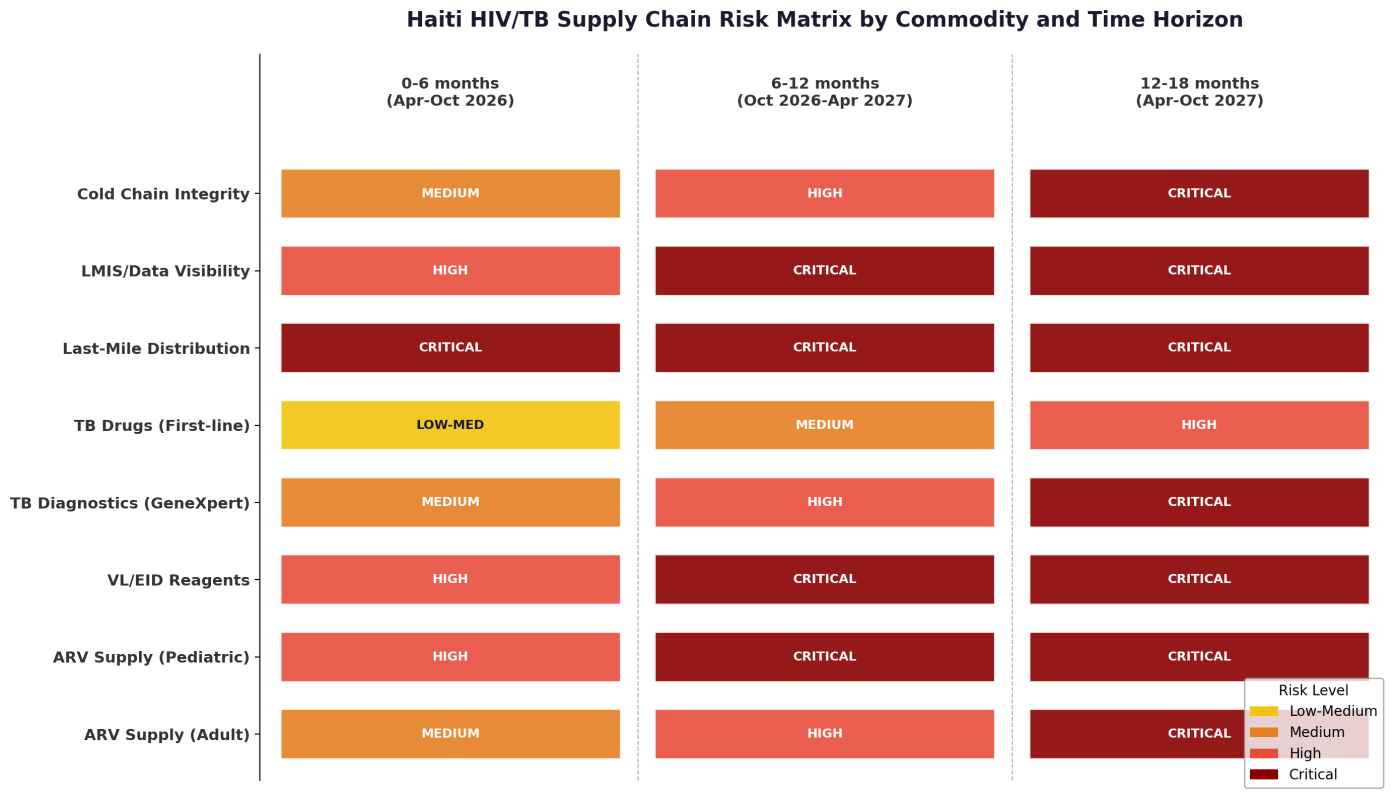
The first thing that fails is distribution. The moment GHSC-PSM ceases operations, the monthly delivery cycle to 272 facilities stops. No other organization in Haiti has the 3PL contracts, the routing knowledge, the security protocols, or the warehouse operations to substitute. The Fleuriot Warehouse, containing millions of dollars in inventory, becomes an inaccessible asset if Chemonics staff depart and the lease lapses. Medicines exist. They simply cannot reach patients.
This is the distinction that gets lost in policy conversations about “procurement mechanisms.” National stock and point-of-care availability are different things. A warehouse full of ARVs in Port-au-Prince does nothing for a patient in Hinche if no truck is coming.
The second thing is viral load and early infant diagnosis testing. The global contracts with Abbott, Hologic, and Roche—which brought Haiti’s per-test cost to $13.50 and included maintenance SLAs—are tied to GHSC-PSM. Without contract management, equipment maintenance stops, reagent supply becomes irregular, and the negotiated pricing disappears. VL testing turnaround times, already described as “unacceptably high” in COP23, will deteriorate further. EID testing for HIV-exposed infants is among the most time-sensitive diagnostics in medicine: a delay of weeks can mean the difference between a treated child and a dead one.
Pediatric ARVs are already in crisis. As of May 2025, Haiti had fewer than six months of stock in two pediatric ARV lines, one of only four countries globally in that position. Pediatric formulations (DTG-10 dispersible tablets, nevirapine suspensions, raltegravir granules) have complex manufacturing, limited suppliers, and long lead times. They are the kind of products that simply do not appear through alternative channels on short notice.
Adult ARVs have a fragile buffer. The emergency flight in February 2025 delivered roughly six months of supply. Haiti’s high multi-month dispensing rate (72% of patients receive 6+ months at a time) provides some patient-level cushion. But this buffer is finite and was calibrated to pre-crisis volumes. It is being drawn down without systematic replenishment.
TB drugs are at lower immediate risk because they flow primarily through PROMESS and the Global Fund track rather than GHSC-PSM. But the “Common Basket” coordination mechanism — intended to unify quantification across both donors — loses its PEPFAR half. And site-level TB drug stockouts were already documented at two facilities in September 2024.
Over the medium term, six to eighteen months, everything compounds. The cold chain fails as maintenance lapses and fuel becomes unavailable. SYGDOCC, the eLMIS, loses technical support; without data, supply planners are blind. The GeneXpert network—already down to only two sites connected via VPN as of May 2024—goes fully offline. TB case detection, already at only 63% in a country with the highest TB incidence in the Western Hemisphere (149 per 100,000), collapses further.
And the cascade begins: patients miss refills, viral loads rebound, resistance emerges, onward transmission accelerates. The 50,000+ people on ART in the West Department alone, identified by UNAIDS as “at high risk of disruption” before the closeout even began, begin falling out of care.
The expected order of failure:
- Last-mile distribution stops (immediate)
- VL/EID testing deteriorates (weeks)
- Pediatric ARV stockouts deepen (already occurring)
- LMIS data goes dark (1-3 months)
- Facility-level adult ARV stockouts begin (3-6 months)
- National adult ARV stocks deplete (6-12 months)
- GeneXpert network goes offline (3-6 months)
- TB case detection collapses (6-12 months)
VII. The Comparative Cruelty of Context
It would be misleading to suggest that the GHSC-PSM transition is only dangerous in Haiti. It is dangerous everywhere. But the nature of the danger in Haiti is categorically different from what Uganda, Zambia, or Mozambique face — and understanding why illuminates something about the limits of the entire global health architecture.
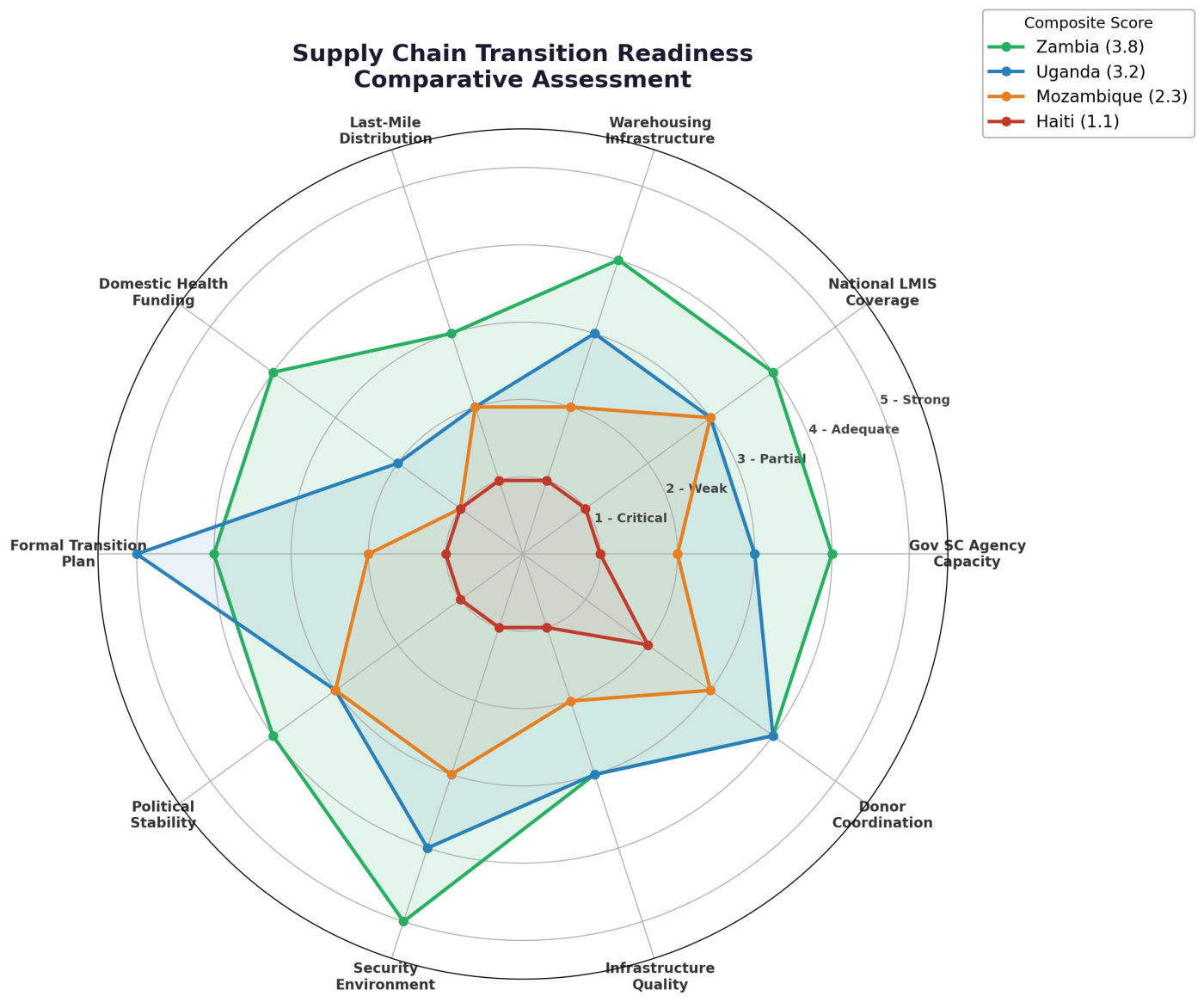
Zambia (composite readiness score: 3.8 out of 5) is the benchmark. ZAMMSA—the national medicines agency—performs at 78-93% across central supply chain functions. Domestic procurement funding reached 52% in 2023. The eLMIS covers nearly every facility. A $362 million Global Fund grant explicitly targets supply chain strengthening. Zambia has problems. It does not have a crisis.
Uganda (3.2/5) occupies an aspirational middle. Its 10-Year Supply Chain Roadmap is the most sophisticated transition plan among comparators. The National Medical Stores has real warehouse capacity: 43,000 pallets. But 77% of ARV financing remains donor-funded, and PEPFAR covered 100% of last-mile transport. When the January 2025 freeze hit, ARV supplies dropped to seven-day rations at some facilities in midwestern Uganda. At one site, babies were born HIV-positive because the warehouse was locked and drugs went undelivered. Uganda has a plan. It is years from executing it.
Mozambique (2.3/5) is the cautionary tale. A 2013 strategic plan for pharmaceutical logistics was never implemented over eleven years. CMAM received legal supply chain authority only in March 2024. A 2025 audit found 87% of facilities with significant stockouts and $15.8 million in expired medicines at the central level. Mozambique has a framework. It has not built the house.
Haiti (1.1/5) is not on the same scale.
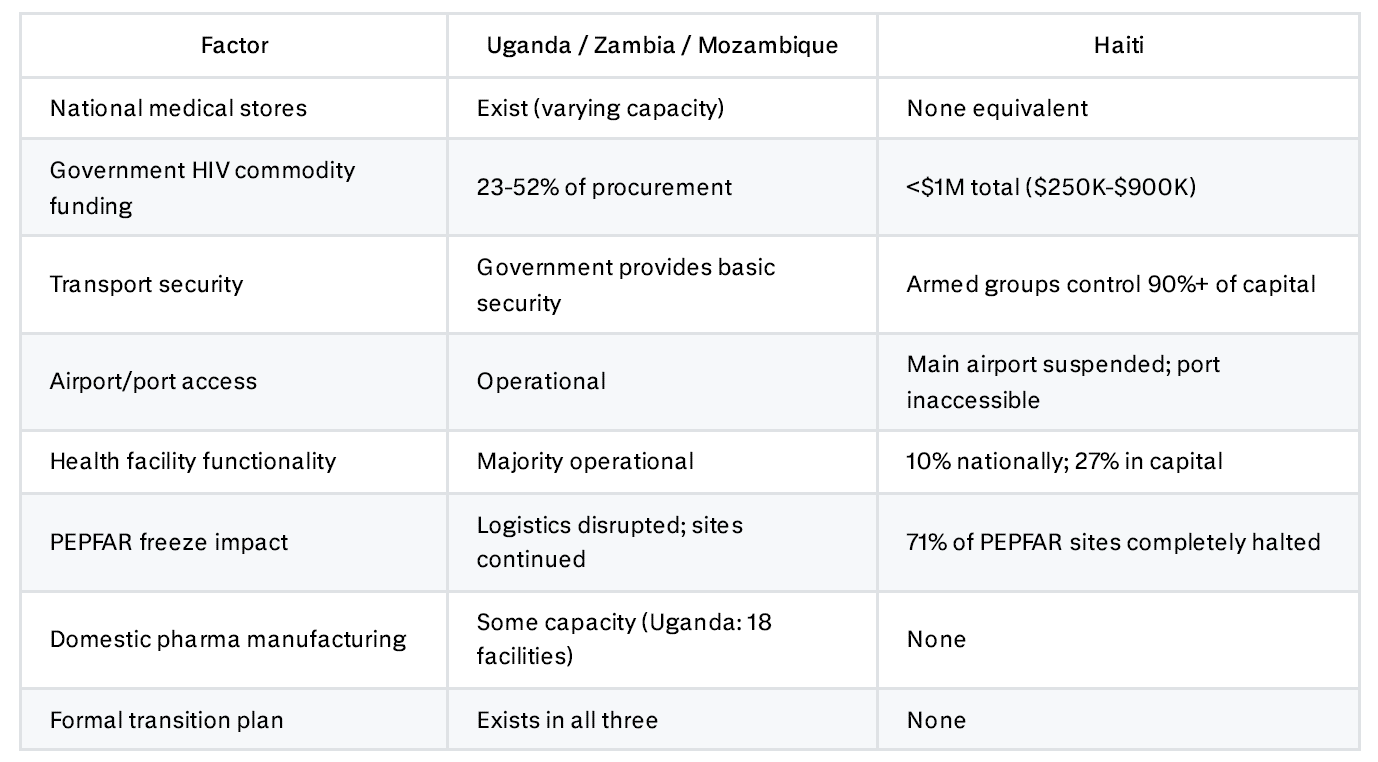
When PEPFAR froze, 128 of 181 PEPFAR-supported sites in Haiti halted completely, that’s a 71% collapse rate. In the African comparators, sites were disrupted but continued operating. The difference reveals something fundamental: in those countries, the government, however weakly, provides a floor. In Haiti, there is no floor. GHSC-PSM was not supporting a national system. It was performing the functions that a national system would perform if one existed.
The distinction matters because transition planning assumes something to transition to. In Zambia, you can design a phased handover to ZAMMSA. In Uganda, you can fund the Roadmap. In Haiti, there is no institution to hand over to, no budget to phase in, no secure corridor to transport through, and—increasingly—no facilities to deliver to.
VIII. The Signals Before the Silence
One of the cruelties of supply chain failure is that it is invisible until it is catastrophic. A patient who receives their last bottle of ARVs does not look different from a patient who receives their next-to-last bottle. The warehouse that dispatches its final shipment looks exactly like the warehouse that dispatched the one before. The system appears functional until, quite suddenly, it doesn’t.
This is why early warning indicators matter — not as an academic exercise, but as the only tool available to detect collapse before it becomes irreversible.
What to Watch Weekly
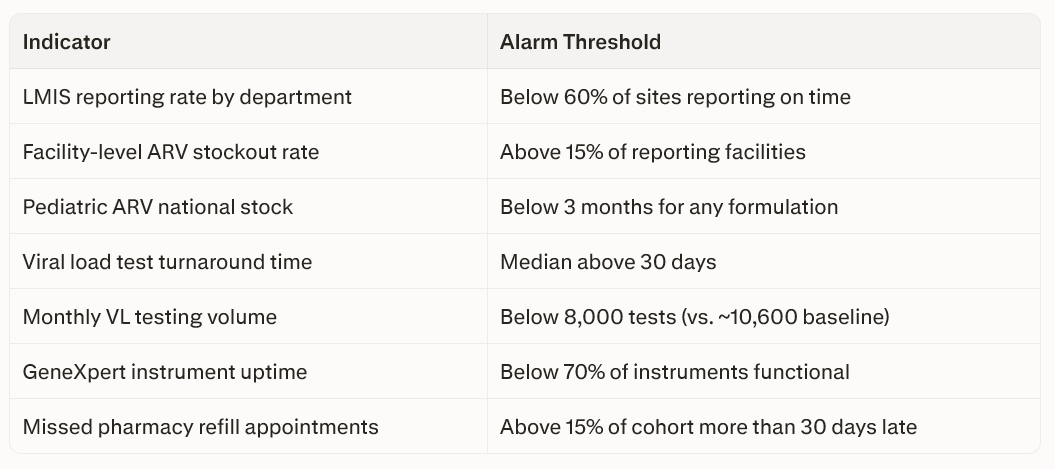
What to Watch Monthly
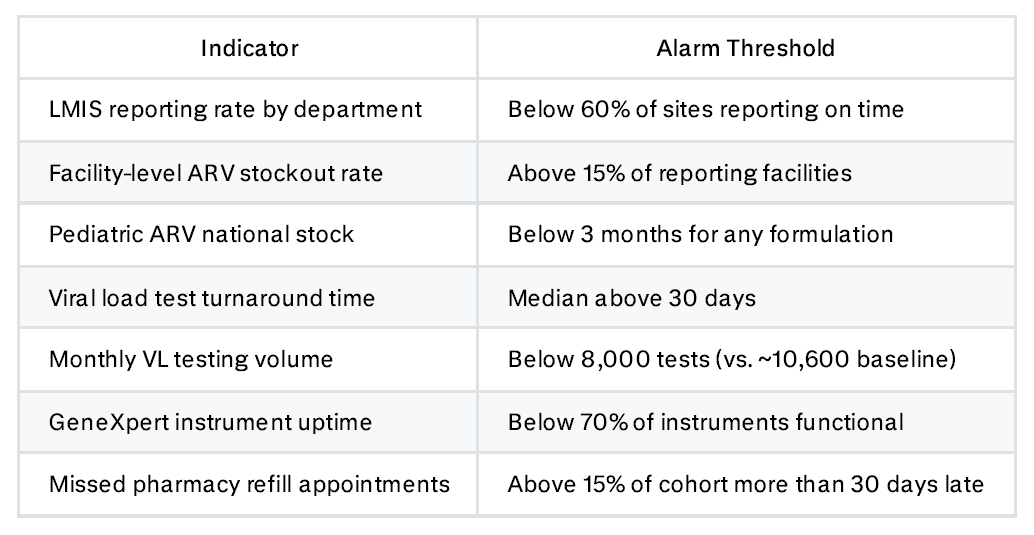
What to Watch Quarterly
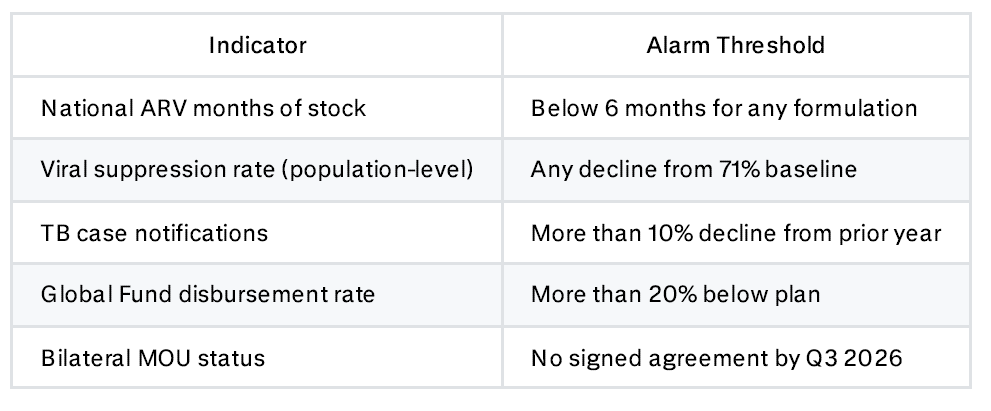
The most critical single indicator is whether the Fleuriot Warehouse is open and staffed. If it closes, everything downstream fails immediately. The second most important is viral load test turnaround time — a sensitive proxy for overall system health that deteriorates early and reflects supply chain problems before they show up in patient outcomes.
IX. Three Futures
Best Case: Coordinated Transition (Probability: ~10-15%)
A bilateral MOU is signed before GHSC-PSM closes. U.S. funds are channeled through the Global Fund or PAHO for procurement continuity. The Fleuriot Warehouse is transferred to a designated operator (perhaps World Vision, perhaps a local 3PL) with bridge funding. The Global Fund Emergency Fund is activated specifically for in-country logistics. WFP and PAHO provide distribution support. SYGDOCC deployment continues under the RSSH grant.
This scenario requires simultaneous coordinated action by the State Department, Global Fund Secretariat, PAHO, MSPP, and World Vision in a gang-controlled operating environment where basic meetings are difficult to schedule. No transition of this complexity has been executed under comparable conditions. As of April 2026, no evidence of this level of coordination has emerged.
Most Likely Case: Fragmented Patchwork (Probability: ~55-65%)
GHSC-PSM closes down over months in a managed but incomplete process. Some stocks are transferred to PROMESS or partners, but without integrated distribution management. The Global Fund expands procurement somewhat, but cannot fill the logistics void. Implementing partners—PIH/Zanmi Lasante, GHESKIO, World Vision—improvise local distribution using their own resources. PAHO provides episodic emergency shipments, as it did with 7.7 tons in February 2025. VL/EID testing degrades. Stockouts hit the most insecure and remote areas first, then spread. Data visibility deteriorates. The emergency ARV buffer is consumed without replenishment.
The outcome: twelve to twenty-four months of degraded but not entirely collapsed service delivery. ART coverage drops from 84% to an estimated 60-70%. VL testing coverage falls sharply. Pediatric programs suffer most. TB case detection dips below 50%. Twenty years of gains erode but are not entirely lost…provided partner organizations can sustain improvised operations long enough for a new arrangement to materialize.
Worst Case: Systemic Disruption (Probability: ~20-30%)
GHSC-PSM closes abruptly. The warehouse lease lapses or the facility is compromised by gang activity; millions in inventory are lost. No distribution mechanism is established before facility stocks run out. VL/EID testing ceases. The GeneXpert network goes offline. Multiple ARV formulations stockout nationally. Implementing partners lose operational funding. The security situation deteriorates further, closing more facilities. Treatment interruption cascades. Viral resistance emerges. Onward transmission accelerates. TB case detection effectively stops.
Haiti’s HIV prevalence—driven below 2% over two decades of sustained work, from over 6% at the epidemic’s peak—begins to reverse.
The worst case does not require a catastrophic event. It requires the absence of coordinated action in a context where coordination is already nearly impossible. Every individual failure (warehouse closure, 3PL contract lapse, cold chain breakdown, LMIS blackout) is independently probable. Their simultaneous occurrence creates a systemic failure that no single actor can reverse.
X. What Is to Be Done
For program managers
The immediate priority is contingency planning for distribution. Map which facilities are reachable by which routes under current security conditions. Identify local transport providers, however compromised their access may be. Pre-position maximum stocks at facility level while the warehouse still operates. Expand multi-month dispensing to twelve months where possible, not best practice, but a survival strategy. Explore direct maintenance and reagent agreements with Abbott, Hologic, and Roche, independent of GHSC-PSM. The per-test cost will be higher. The alternative is no testing at all.
For PEPFAR and the U.S. government
The highest-impact single action is keeping the Fleuriot Warehouse operational—through a new contract, a Global Fund transfer, or a bridge arrangement with Chemonics. Losing the warehouse means losing the physical infrastructure on which everything depends. Any bilateral MOU must include specific provisions for in-country logistics, not just commodity procurement. An agreement to buy ARVs through the Global Fund, but not to fund their delivery in Haiti’s security environment, is an agreement to procure medicines that will sit in a building.
For the Global Fund
The Emergency Fund should be activated proactively for in-country logistics—a function outside the Fund’s normal scope, but one the crisis demands. The GC8 allocation process should treat Haiti as a special case requiring logistics funding beyond normal parameters. The wambo.org platform issues need urgent resolution.
For implementing NGOs
PIH, GHESKIO, CMMB, and others need to prepare for a period where they function as de facto supply chain operators in their catchment areas, a role for which they were never designed or funded. Build emergency stockpiles. Coordinate with WFP and the Logistics Cluster on distribution alternatives. Prepare community-based dispensing protocols. And document everything! Because the amfAR finding that bilateral MOUs lack measurable metrics means that implementing partner data may be the only accountability mechanism available.
XI. Coda: The Architecture of a Preventable Catastrophe
There is something revealing about the phrase “supply chain transition.” It is the language of managed change — orderly, planned, sequential. It assumes a handover from one functioning system to another. It assumes institutional capacity to receive what is being handed over. It assumes, at a minimum, the existence of roads that trucks can drive on and warehouses that staff can enter.
None of these assumptions hold in Haiti.
What is occurring is not a transition. It is the withdrawal of a system with no successor in place, no institutional capacity to absorb its functions, and no operating environment in which conventional alternatives can function. The reference brief that grounds this analysis states it precisely: “The situation represents a supply chain continuity risk rather than a pure funding gap.”
Money can be redirected through the Global Fund, through PAHO, through bilateral channels. But money does not drive trucks through gang checkpoints. Money does not maintain cold rooms during power outages. Money does not negotiate passage through Viv Ansanm territory. Money does not deliver dolutegravir suspensions to a health center in Plateau Central accessible only on foot—which is what Zanmi Lasante staff have done, repeatedly, because the road was blocked and the patients were waiting.
Haiti is the most supply-chain-dependent country in the world by USAID funding share, with the lowest institutional capacity, the worst security environment, and no signed transition agreement. The expert consensus—from CGDev, from CSIS, from KFF, from UNAIDS, from Partners In Health, from the journalists tracking the closeout in real time—is unambiguous: without deliberate, coordinated, and rapid intervention, the second half of 2026 will see Haiti’s HIV and TB programs enter a period of systemic degradation from which recovery will take years and cost lives.
The early warning indicators are already flashing. Pediatric ARV stocks are in shortage. Viral load turnaround times are “unacceptably high.” Two TB treatment sites ran out of drugs in September 2024. LMIS reporting rates are below target. The GeneXpert network is functionally disconnected. And the institution that held all of this together, however imperfectly, however dependent on foreign money and foreign management, is being wound down.
There is a warehouse in Port-au-Prince. It is still open, as of this writing. The women who run it still show up. The trucks still leave when the roads allow it. The cold room still hums at 2-8°C.
The question is, for how long.
⎯
Dr. Alain Casséus currently serves as Infectious Diseases Division Chief and Principal Investigator for the PEPFAR Project at Zanmi Lasante, PIH’s sister organization in Haiti. Dr. Casséus has worked with ZL since 2007, with a primary focus on HIV/TB and improving care through research. In his nearly two decades working in Haiti, he has led massive vaccination campaigns, conducted cross-organizational research, and ensured thousands of HIV patients have received care - by his hand and others.

